@trophywench I was getting hospital phone physio of very little help, we’d never met and each Physio wanted background details taking up much of the time. Coincidentally the department manager left to work in a private clinic near our home. I see her once a month for an hour, she’s brilliant worth every penny although she doesn’t take prisoners so it’s hard work with sheets of activities to do at home. My calf muscle had almost disappeared, both legs had hardly been used for several weeks but they are now.I can't help cos I don't have one either ! Mine's usually in the low 50s, 53 ish, though sometimes goes up a bit. I happened to have an A1c a few weeks after I did my knee which was by no means ideal as the last 4 weeks prior to visiting the vampire, has the most effect on the total result - and not at all surprisingly it had shot up to 64. Came back down again to 57 and then back to 53 by 6 and 12 months after.
If you are still suffering pain and discomfort from your breakages and hence lack of exercise generally this could affect your A1c too. Are you getting any physio for the leg or not?
Just wondering if the ones they had me doing - lying sat up on the bed! - would do you any good, because they work all your leg muscles above and below the knees and therefore also help more than a bit with circulation of oxygenated blood so excellent for healing and assisting prevention of arteries getting any harder if they are.
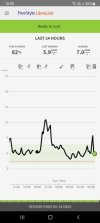
My recent Hba1c was 66, 64 last year so it does seem high and yet my time in target isn’t bad (or so I thought) it seems my Libre A1c wasn’t a good indicator. We have never been cake, biscuit or pudding eaters so I didn’t need to cut them down. After reading the menus from other members I was quite shocked as I wouldn’t ever have eaten most of those foods but it’s given me some ideas for a bit more variety in future.
 One of those many things I'd never bothered finding out about cos formerly on a 'need to know' basis, I never had !
One of those many things I'd never bothered finding out about cos formerly on a 'need to know' basis, I never had !