There is certainly more than one thing that can cause high blood pressure. Visceral fat is one of them. I've lost 12.5 pounds so far. Saw my doctor yesterday. my BP was 99/64 so she's advised me to cut my tablets in half going forward. Some days I don't bother with a tablet at all. I'm hoping that 25 lbs from now I'll be off my Losartan altogether. I also have atherosclerosis so...stiff arteries and that doesn't help flow thru the pipes.Just talking about blood pressure here. Yes, clearing visceral fat can reverse T2D as it did for me. But I haven't seen much on the extent to which visceral fat is a BP driver independent of overall body fat.
-
Please Remember: Members are only permitted to share their own experiences. Members are not qualified to give medical advice. Additionally, everyone manages their health differently. Please be respectful of other people's opinions about their own diabetes management.
-
Take a look at our new Type 2 Diabetes Remission section on the Diabetes UK website: https://www.diabetes.org.uk/diabetes-the-basics/type-2-remission
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Weight loss rate and remission
- Thread starter PerSpinasAdAstra
- Start date
- Status
- This thread is now closed. Please contact Anna DUK, Ieva DUK or everydayupsanddowns if you would like it re-opened.
nonethewiser
Well-Known Member
- Relationship to Diabetes
- Type 1
There is certainly more than one thing that can cause high blood pressure. Visceral fat is one of them. I've lost 12.5 pounds so far. Saw my doctor yesterday. my BP was 99/64 so she's advised me to cut my tablets in half going forward. Some days I don't bother with a tablet at all. I'm hoping that 25 lbs from now I'll be off my Losartan altogether. I also have atherosclerosis so...stiff arteries and that doesn't help flow thru the pipes.
Weight loss is big factor in lowering BP as is exercise.
My wife always had low BP even before losing 5 stone, thankfully it didn't lower much further but weight loss did rid her body of visceral fat & got rid of her predicates diagnosis, so was certainly worth every effort.
congrats to your wife. Weight loss any way you can do it is key.Weight loss is big factor in lowering BP as is exercise.
My wife always had low BP even before losing 5 stone, thankfully it didn't lower much further but weight loss did rid her body of visceral fat & got rid of her predicates diagnosis, so was certainly worth every effort.
PerSpinasAdAstra
Well-Known Member
- Relationship to Diabetes
- Type 2
- Pronouns
- He/Him
Here's screenshots of the BP and BG readings I referred to. The drop in evening BP readings is fairly dramatic. Exercise levels, diet, salt and water intake were unchanged. The conclusion I've drawn is I burned off some fat in just the right spot, though I'd agree that it's hardly conclusive evidence.
Attachments
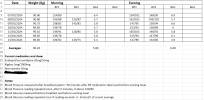
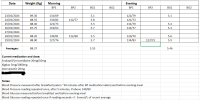
Here's something to look at: https://www.ahajournals.org/doi/full/10.1161/01.hyp.27.1.125#:~:text=The changes in both visceral,the changes in mean BP. Quote from the study: "The changes in both visceral fat area and V/S ratio were significantly correlated with changes in mean BP. However, the changes in weight, BMI, waist-to-hip ratio, and subcutaneous fat area were not correlated with the changes in mean BP" I don't think this is controversial.Here's screenshots of the BP and BG readings I referred to. The drop in evening BP readings is fairly dramatic. Exercise levels, diet, salt and water intake were unchanged. The conclusion I've drawn is I burned off some fat in just the right spot, though I'd agree that it's hardly conclusive evidence.
Yes and ironically dietary fat is handled quite easily because it doesn't spike insulin. The clogging problem comes when too many carbs flood in, insulin spikes telling the liver to make fat, which it does, and subsequently shoves it into places it shouldn't go ater it runs out of the right places. Prof. Taylor's twin cycle explanation of this is nothing less than brilliant.Deleted Member 45380 said:
Last edited by a moderator:
Eddy Edson
Well-Known Member
- Relationship to Diabetes
- In remission from Type 2
Poking around, there are a lot of individual studies of varying size and quality suggesting close associations between visceral / perirenal fat and hypertension. What you really want to see are large-scale metastudies and expert reviews seeking to adjust for confounders, biases etc over large datasets & support causality, and on a quick look I still don't find much along those lines.Here's screenshots of the BP and BG readings I referred to. The drop in evening BP readings is fairly dramatic. Exercise levels, diet, salt and water intake were unchanged. The conclusion I've drawn is I burned off some fat in just the right spot, though I'd agree that it's hardly conclusive evidence.
But this seems like a detailed recent review: https://academic.oup.com/ckj/article/17/1/sfad282/7419873
In 1988, Gerald Reaven hypothesized that insulin resistance was the key factor in a group of metabolic disorders, later called ‘Syndrome X’, which included impaired glucose tolerance (IGT), hyperinsulinemia, high triglycerides, low high-density lipoprotein cholesterol levels and hypertension [23, 24]. Then Norman Kaplan identified also central obesity as a key driver of CVD and defined the cluster of visceral obesity, IGT/insulin resistance, hypertriglyceridemia and hypertension as the ‘deadly quartet’ [25]. For more than 30 years, insulin resistance and hyperinsulinemia-dependent overstimulation of sympathetic nervous system (SNS) and increased renal sodium reabsorption have been considered as primary mediators of elevated BP in metabolic syndrome and obesity. However, strong experimental and clinical evidence is available to suggest that obese subjects can be normotensive despite severe insulin resistance and hyperinsulinemia [26]. Indeed, increased renal sodium reabsorption and consequent expanded plasma volume sustained by compression of the kidney by perirenal and intrarenal fat and systemic/renal SNS and renin–angiotensin–aldosterone system (RAAS) overactivation have been subsequently identified as major factors mediating the initiation of hypertension in obesity [5, 26]. On the other hand, it is clear that in the long term, insulin resistance and hyperinsulinemia, and consequent hyperglycemia and dyslipidemia, interact synergistically with elevated BP in the induction of renal and vascular injury that in a ‘vicious circle’ contribute to further worsening of hypertension and increased risk of renal and cardiovascular complications.
This suggests that (a) kidney fat can indeed be a main driver for hypertension but also (b) it can happen in the absence of insluin resistance, which suggests that you can get kidney fat without liver fat, at least in the short term.
Anyway, it's all very interesting.
Eddy Edson
Well-Known Member
- Relationship to Diabetes
- In remission from Type 2
For some reason I forgot to check out AHA scientific statements, usually a great resource for detailed evidence reviews. This from 2021: https://www.ahajournals.org/doi/10.1161/HYP.0000000000000202
The pathophysiology of obesity hypertension is multifactorial and highly time dependent (Figure 1). Overfeeding humans and experimental animals rapidly activates the sympathetic nervous system (SNS) and renin-angiotensin-aldosterone system (RAAS), even before large increases in body weight occur.15–18 Conversely, decreased caloric intake resulting from voluntary food restriction or MS rapidly reduces BP and attenuates metabolic disorders in most patients with obesity, including those with type 2 diabetes.15,19 Although increases in BP that accompany excess weight gain are initially mild, with chronic obesity, there is gradual injury to target organs that exacerbates hypertension. The long-term impact of obesity on BP also depends on where excess fat is stored, with visceral fat conveying a greater risk for hypertension than subcutaneous fat.20,21
One of the references is from 2014 with data from the large, high-quality Dallas Heart Study:
Methods:
Normotensive participants enrolled in the Dallas Heart Study were followed for a median of 7 years for the development of hypertension (systolic blood pressure [SBP] ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg, or initiation of blood pressure medications). Visceral adipose tissue (VAT) and subcutaneous adipose tissue (SAT) was quantified by magnetic resonance imaging and proton-spectroscopic imaging, and lower body fat (LBF) was imaged by dual-energy x-ray absorptiometry. Multivariable relative risk regression was performed to test the association between individual fat depots and incident hypertension, adjusting for age, sex, race/ethnicity, diabetes, smoking, SBP, and body mass index (BMI).
Conclusions:
Increased visceral adiposity, but not total or subcutaneous adiposity, was robustly associated with incident hypertension. Additional studies will be needed to elucidate the mechanisms behind this association.
Weight-Loss Strategies for Prevention and Treatment of Hypertension: A Scientific Statement From the American Heart Association
Increased visceral adiposity, rather than subcutaneous adiposity, is robustly associated with incident hypertension. ...The pathophysiology of obesity hypertension is multifactorial and highly time dependent (Figure 1). Overfeeding humans and experimental animals rapidly activates the sympathetic nervous system (SNS) and renin-angiotensin-aldosterone system (RAAS), even before large increases in body weight occur.15–18 Conversely, decreased caloric intake resulting from voluntary food restriction or MS rapidly reduces BP and attenuates metabolic disorders in most patients with obesity, including those with type 2 diabetes.15,19 Although increases in BP that accompany excess weight gain are initially mild, with chronic obesity, there is gradual injury to target organs that exacerbates hypertension. The long-term impact of obesity on BP also depends on where excess fat is stored, with visceral fat conveying a greater risk for hypertension than subcutaneous fat.20,21
One of the references is from 2014 with data from the large, high-quality Dallas Heart Study:
Objectives:
This study sought to determine the relationship between adipose tissue distribution and incident hypertension.Methods:
Normotensive participants enrolled in the Dallas Heart Study were followed for a median of 7 years for the development of hypertension (systolic blood pressure [SBP] ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg, or initiation of blood pressure medications). Visceral adipose tissue (VAT) and subcutaneous adipose tissue (SAT) was quantified by magnetic resonance imaging and proton-spectroscopic imaging, and lower body fat (LBF) was imaged by dual-energy x-ray absorptiometry. Multivariable relative risk regression was performed to test the association between individual fat depots and incident hypertension, adjusting for age, sex, race/ethnicity, diabetes, smoking, SBP, and body mass index (BMI).
Results:
Among 903 participants (median age, 40 years; 57% women; 60% nonwhite; median BMI 27.5 kg/m2), 230 (25%) developed incident hypertension. In multivariable analyses, higher BMI was significantly associated with incident hypertension (relative risk: 1.24; 95% confidence interval: 1.12 to 1.36, per 1-SD increase). However, when VAT, SAT, and LBF were added to the model, only VAT remained independently associated with incident hypertension (relative risk: 1.22; 95% confidence interval: 1.06 to 1.39, per 1-SD increase).Conclusions:
Increased visceral adiposity, but not total or subcutaneous adiposity, was robustly associated with incident hypertension. Additional studies will be needed to elucidate the mechanisms behind this association.
PerSpinasAdAstra
Well-Known Member
- Relationship to Diabetes
- Type 2
- Pronouns
- He/Him
Many thanks for those @Eddy Edson
It would seem from your posts and some reading I've done myself tonight that there is a strong link between visceral adipose and renal ectopic fat and blood pressure, but that it's not a nice simple linear relationship. As such I definitely won't be able to use BP changes as a reasonable way to gauge reductions in fat in and around my liver and pancreas. The sudden drop in BP is a good sign that I'm well on the way to losing fat in the right places, but BP changes won't tell me when I'm 'there'. It seems I'm back to daily blood glucose tests, and HbA1c tests taken months after the event, to help inform me where the 'danger zone' might be as regards my body weight. That's assuming I achieve remission in the first place, and that the 'personal fat threshold' hypothesis is correct.
It would seem from your posts and some reading I've done myself tonight that there is a strong link between visceral adipose and renal ectopic fat and blood pressure, but that it's not a nice simple linear relationship. As such I definitely won't be able to use BP changes as a reasonable way to gauge reductions in fat in and around my liver and pancreas. The sudden drop in BP is a good sign that I'm well on the way to losing fat in the right places, but BP changes won't tell me when I'm 'there'. It seems I'm back to daily blood glucose tests, and HbA1c tests taken months after the event, to help inform me where the 'danger zone' might be as regards my body weight. That's assuming I achieve remission in the first place, and that the 'personal fat threshold' hypothesis is correct.
Eddy Edson
Well-Known Member
- Relationship to Diabetes
- In remission from Type 2
My personal rough'n'ready indicator is fasting BG. While this is in the 4's then it probably means no hepatic insulin resistance => no liver fat => probably no pancreas fat => everything normalised.Many thanks for those @Eddy Edson
It would seem from your posts and some reading I've done myself tonight that there is a strong link between visceral adipose and renal ectopic fat and blood pressure, but that it's not a nice simple linear relationship. As such I definitely won't be able to use BP changes as a reasonable way to gauge reductions in fat in and around my liver and pancreas. The sudden drop in BP is a good sign that I'm well on the way to losing fat in the right places, but BP changes won't tell me when I'm 'there'. It seems I'm back to daily blood glucose tests, and HbA1c tests taken months after the event, to help inform me where the 'danger zone' might be as regards my body weight. That's assuming I achieve remission in the first place, and that the 'personal fat threshold' hypothesis is correct.
Took me ~6 months to get to that point. Steady for the last 5 1/2 years now.
- Status
- This thread is now closed. Please contact Anna DUK, Ieva DUK or everydayupsanddowns if you would like it re-opened.