No need to be concerned about what doses other people need.
I know, but it's just such a difference.
I would find it hard to do a full day free of carbs,
That's a good point. I'm starving by 2pm! I've had a carb free morning this morning with 18 units of Tresiba for the last 2 nights. I'm sitting stable this morning after only scrambled eggs and a coffee. I'll go for a carb free dinner and see how I feel at tea time where I will probably have some carbs and do a careful dose of NovoRapid.
Do you have a half unit pen.
I don't but I plan on asking about this when I next go. I have asked for one in the past, but they kept saying "you don't need one of those". I always thought it was better to always have the option than not.
Do ask for a half unit pen - they’re so useful.
As above ^
I'd recommend you get yourself a half unit pen for your novorapid, they're really useful- i have the echo which has a display of how much you last injected and how long ago it was, great if you forget or think you made a mistake. Also more robust and take up less fridge space than disposables, just ask it to be presvribed. Ask for a spare too.
I've not heard of Echo no, but this sounds really good and helpful! I'll definitely be asking about this when I get my appointment. Thank you.
According to abbots own literature you shouldn't make treatment decisions on libre readings alone, always check with finger prick.
I've gone back to fingerpricks now and use the CGM only to alert me to lows/highs earlier so I can then finger prick and and go by how I feel to act if needed. I think for me, it may be a small case of the CGM providing me too much information and me fixating on it more than I need to. Particularly the down arrow that makes me feel a little anxious when I see it saying down and I'm like 5.5. I then just think "avoid the low!"
there was some discussion on hear to say it can now be calibrated, which would make it even more useful.
I wasn't aware of this. I'll look into it.
I was on this before they moved me over to Tresiba, as I was having (at least I/we thought) issues with it...
and I take it twice a day, so the tail end of each dose overlaps with the build up of the next dose. It had a peak of activity and a slow tail off. You can adjust the day and night time doses independently to cover what you need or don't need and you can adjust the timing of the doses to provide that peak of activity when you need it most. It is much more flexible than Tresiba so you can adjust it daily whereas Tresiba needs 3 days before you see the full effect of any change and decide whether or not you need to change it again.
...but now I know this, I'll discuss this with them when I get in. I wasn't aware also that Tresiba needs 3 days to take effect of changes. So I've spent the last 2 nights doing 18 from 20. I'm probably not going to see the effects of that yet, at least until tomorrow? I guess it makes no difference what time I'm doing this at that to help them coming down in ther night.
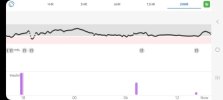
On the point of going down in the night, they don't drop drastically, and the CGM tends to alarm me around the time of waking up anyway most of the time. It's more that, at night, I'm aware it does this, so I tend to run bloods a little higher to compensate for this at night. See screenshots below of the last 2 nights to mornings and how it drops. I feel like I then just get into a wrestling match with it for the rest of the day from the morning - unless, I have a completely carb free breakfast.


As regards the clinic, I wonder if they have a helpline you can ring.
I'm at an appointment with the diabetic nurse in my practice today so I'm going to air all my problems, issues and concerns, and ask about this.
Did you set it up so that the hospital has access to your data via LibreView? Usually this involves inputting a code for your particular hospital clinic, which then allows them to access it so that they can look at it and advise you if you have a problem.
I wasn't aware this was possible. Again, I will ask about this today and which clinic code I need.
Sorry to write so much but there were quite a few things that your post highlighted that I wanted to comment on and explain and no doubt whilst I have been typing others will have covered some/all of them anyway..... I am busy cooking tea so I keep leaving the computer and coming back to it hence it has taken me a long time to compose. 🙄
Better that than what I've just done - spent half an hour writing a response, to accidentally hit the back button on my mouse and lose it all! I've had to type all this back out again
😱
I appreciate the long message also it allows me to read all at once as I find it hard to get time with work. So thank you for being so detailed.
Who advised you that you need to speak to a professional before changing doses?
The professionals themselves. It's referring to my basal, not bolus. I know bolus depends on what you're eating at the time. But I was told to speak with them before adjusting my Tresiba. I think the reason why makes more sense after the info from
@rebrascora about the Tresiba length of activity. I'll question this more when I go in today and when I get the clinic appointment.
Thank you all so much for the comments. I feel more armed with knowledge and questions that could set me down a better path with this now.
I have the appointment at 1pm today, so I'll try to find time to check back in later and let you know how things go.
Have a good day all.