Proud to be erratic
Well-Known Member
- Relationship to Diabetes
- Type 3c
- Pronouns
- He/Him
Hi Judy,Hi,thank you for your reply.
I’m still very up and down. Had my bloods (lfts) done before Xmas,came back borderline,had them re- done,came back abnormal. Doctor rang me,wants to re-do them again on Monday,if they come back as high again then he is getting in touch with my consultant for advice. Doctor thinks it could be a short stay in hospital,put on a drip to repair my liver.Hopefully it doesn’t come to that.
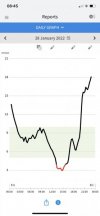
Really sorry you are very up and down. I am also still pretty erratic sometimes; indeed only yesterday I realised that I haven't had a single day 100% in range since October. But my overall time in range is gradually improving; still very slow work in progress. Sometimes I know what the cause is and sometimes I simply don't have a clue. Below is me over the last 24 hrs. The tiny 7.8 in the top left is Diabox giving my BG at that moment (by chance = my libre reading, not always so close).

And this is what I see on Diabox, 5 mins later BG=8.2 and climbing slightly. Each dot is a reading from every 5 mins and this screen is displaying the last 12 hrs (my choice, could have been 1, 3, 6, 12 or 24 hrs). The mild rise didn't actually happen, I know to not react to possible mild change.

If I scroll further down that D'box screen, below, I can remind myself that I have my non-urgent high alarm set for 10 (Urgent high alarm is normally 15 and I would usually take a correction bolus at that point). The routine low alarm is set for 6.2, which I just monitor happy to be below that when change is gentle (the 26% reflects time below 6.2, not below 4, but if I want that I just set the upper low alarm at 4 and the % will change - today nil so far) and the Urgent low alarm is routinely at 4.2 and I'm scrambling for JBs if the Urgent low siren goes!

The Std deviation, GVI & PGS are interesting (bottom of screenshot above) fairly reflecting my Glucose Variability Index (GVI) is poor; to be expected with no pancreas and consequent brittle diabetes. My challenge to myself this year is to improve that GVI.
Before my pancreatectomy I had a stent fitted to bypass the bile duct blockage from the tumour. The relief to my deep jaundice was almost instant - quite amazing. But during the procedure they nicked my liver, unfortunately. I started to feel off and getting worse daily, but didn't realise my liver had been damaged. Just before Xmas I spoke on the phone to my nominated cancer nurse and she fobbed me off; I accepted that, slightly unhappily. On 2 Jan 20 I had to have a CT scan prior to my forthcoming surgery, and felt very ill. I insisted there was something wrong, spoke to & immediately got seen by the senior cancer spec nurse who was able to see my scan results from 45 mins prior and immediately spotted the liver infection on the scan. A blood test identified the specific culprit and 24 hrs later I was on appropriate antibiotics. By this time I was seriously ill, but the abx did their stuff and recovery was pretty swift. So I totally empathise with having a liver problem and if those circumstances recurred I would not allow someone to fob me off again - and insist on being taken seriously.
Regarding your current difficulties: during the night I am anything from 7 to 4. But each night can be quite different. Firstly I recently reduced my basal Tresiba from 11 to 10 and the outcome from that shows particularly well on Diabox. Previously I was making sure I was close to 9 before going to sleep, knowing that my basal would drag me down during the night; after allowing 3 days for the Tresiba change to take effect my night variability is a lot better (as I hoped). Secondly if I'm close to 10 or above I'll take a correction bosul dose before going to sleep; I always finger-prick before that correction, and then exercise judgement on how much correction trying to get to 6 through the night. I rarely hear the upper alarm during the night, but have the volume setting so that the Urgent low alarm always wakes me; so even if I'm overcorrected I get woken up. Sometimes Libre shows I've had a low glucose event during the night, but I'm pretty sure that I haven't. It's just the inherent inaccuracy of the sensor and sometimes the sensor failing.
Your night hypos are bad, too close to problematic for comfort. If your basal is too high overall, then during the night it will drag you too low; presumably you take Tresiba 1x daily - is that morning or evening? You might be worsening things by applying correction if your basal is wrong. I'm not qualified to give medical advice, but as a principle it must be better to sleep safely, albeit a little high than to go hypo while asleep. Internal damage from being too high isn't ideal, but in short bursts I think it's OK, particularly if below, say, 13 or even 15.
I can't remotely explain why you wake up in the 12-15 range after a night hypo and only 2x JBs (c.10gm CHO). Does your Librelink screen shot show an identifiable trend, eg the time and duration of hypo, and the response from JBs? Do you keep a log of what your evening meal was for those occasions? Does that log include absolutely everything? I am mindful that you aren't yet carb counting (and when you start it takes a while to get things about right, so there will be hiccups initially); so the reality is that your pre-bosul isn't matched to your carb intake and the time between bosul and food digestion isn't matched to the GI of what you've eaten. So a rich low GI meal might not start digesting for 3 hrs ... and then your insulin might time lapse after 4 hrs or longer, depending on your natural insulin resistance. It's pretty complicated already and there are still 35+ factors that can play tricks with your BG. But, possibly the real culprit here is medical induced stress - is your liver playing up during the night?
There is something called the Dawn Phenomena (DP) or Foot on the Floor response, which elevates BG on first wakening? I, naively, wrote on this forum before I'd got Libre that I didn't get the dawn phenomena; I was wrong! I now can clearly see this response on my BG most early mornings. I thought no pancreas and thus no glucagon hormone meant my liver couldn't receive any instruction to open the glucose store, but it does. This doesn't happen to everyone, but is fairly common and apparently is a product of evolution and our innate response to go mammoth hunting before breakfast! If you want to know more about this just search for Dawn Phenomena in this forum (top right corner of the page). However this for me is 2 mmoL/L and it often dissipates before I take my first bolus. The questions that intrigue me about the Dawn Phenomenon are: which hormone is triggering this (and how/why)? Why does it sometimes dissipate but not always? Why does it happen sometimes, but not always? Why can I sometimes get 2 hits, when I wake in the small hours and need the bathroom, then later when I wake to get up? One day I'll try to nail down more about this, but what I've read so far has not helped; but it's not so important - it exists for me, sometimes. It could be a small part of the explanation for you.
I strongly suggest you ask your DSN to look at your LibreView and advise you accordingly. I'm presuming you had to establish LibreView and provide the hospital diabetes team with access to your data - as a condition of being fitted with Libre. There are a number of factors in this bit of the jigsaw, for each time this has occurred? If you don't already keep a detailed log I suggest start now - either on a phone or computer OR just on paper. Record as much as you can: exactly what you are eating and drinking, particularly in the evenings; prebolus detail and meal start time. What time you go to bed (routinely take a Libre scan) how long roughly before you fall asleep (scan again) (I can spend an hour reading before sleeping); any night excursions (bathroom or hypos) (scan again), when, what response, etc. You and your DSN are trying to find a pattern or common denominator for your hypos - my DSN made useful adjustments to my DM management from fortnightly scrutiny of photos of my manually completed logbooks, sent by email during lockdown. Record finger pricks, but for hypos scan as your first response and treat, then finger prick.
Finally consider raising your night time alarm to 4.5 at least, if necessary even higher. You need to get ahead of the hypos and better to be woken (disturbed) to fend off the potential hypo. Broken sleep is far from ideal, but in my opinion far better than hypo while sleeping.
Again, this is far too long ... but stick with it, stay strong and contact your DSN ASP.