anniemillie
New Member
- Relationship to Diabetes
- Carer/Partner
- Pronouns
- She/Her
Hi, this is my first post. Strap in it’s a long one!
My father in law (86) has been diabetic for 30
years, first type 2 then type 1. He’s also the only person I’ve ever known who has survived pancreatic cancer. He had his pancreas removed about 10 years ago. He has managed it really well and is very conscientious about his diet.
He’s been on dialysis due to end stage kidney failure for the last year. Again he’s been very conscientious about the foods he should avoid and has generally been coping very well.
Twice in the last six months, his dialysis lines have got infected. As they’re a direct path to his veins, this has resulted in sepsis. The first time didn’t affect him too badly long term but the second, about 6 weeks ago, seems to have really affected him.
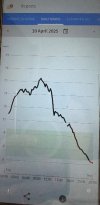
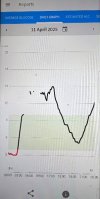
His blood sugar is all over the place. He’s been in and out of hospital about 10 times. (The longest he’s managed with going in is about 36 hours). He’s had two fairly long stays but most of the time they check him over, tell him he’s fine and kick him out (once at 3am with a blood sugar level of 3 but that’s a separate issue) He’s had his insulin changed but the pattern seems to be that his blood sugar rises all day then plummets overnight. He currently spends about 12% of the time in the dangerously low zone and has been down as far as 2.4 according to his Libre device.
The hospital keeps dismissing it as him not managing it properly but he is (or he’s trying to at least). I think they think he’s old and his memory’s failing but he’s sharp as a tack and has about 20 years’ experience of injecting. He’s had moments of confusion due to the hypos but is generally very with it when lucid.
We live 3 hours away and there’s no other family (we’re taking steps to address this but that’s a separate issue). He can’t come to stay with us due to his dialysis. I can work from home (my husband can’t) so have stayed with him for a few days to try to get him back on an even keel but have commitments at home that mean I have to come back after a couple of days and even with really close supervision, it’s still happening.
The diabetes team have now told us to tolerate the highs to help avoid the lows so he’s not having any corrective doses of insulin after his evening meal. I’m writing this at 5am as I’ve been up with him four times and have now given up on sleep. Overnight (when his blood sugar usually drops very low) he hasn’t dipped below 27. It hasn’t changed since 3pm yesterday despite 5 units of Novorapid at 1pm with a small lunch and 8 units at 6pm when he again had a small meal. These amounts are what he has now been told to take and are dependent on his pre-meal blood sugar level. He’s drinking as much as his dialysis team allow him.
There has to be something underlying causing this but the hospital just don’t seem to want to know. They say they’ve run tests and there is nothing. We’re at a loss as to what to try next. Does anybody have any thoughts / experience of something similar please?
My father in law (86) has been diabetic for 30
years, first type 2 then type 1. He’s also the only person I’ve ever known who has survived pancreatic cancer. He had his pancreas removed about 10 years ago. He has managed it really well and is very conscientious about his diet.
He’s been on dialysis due to end stage kidney failure for the last year. Again he’s been very conscientious about the foods he should avoid and has generally been coping very well.
Twice in the last six months, his dialysis lines have got infected. As they’re a direct path to his veins, this has resulted in sepsis. The first time didn’t affect him too badly long term but the second, about 6 weeks ago, seems to have really affected him.
His blood sugar is all over the place. He’s been in and out of hospital about 10 times. (The longest he’s managed with going in is about 36 hours). He’s had two fairly long stays but most of the time they check him over, tell him he’s fine and kick him out (once at 3am with a blood sugar level of 3 but that’s a separate issue) He’s had his insulin changed but the pattern seems to be that his blood sugar rises all day then plummets overnight. He currently spends about 12% of the time in the dangerously low zone and has been down as far as 2.4 according to his Libre device.
The hospital keeps dismissing it as him not managing it properly but he is (or he’s trying to at least). I think they think he’s old and his memory’s failing but he’s sharp as a tack and has about 20 years’ experience of injecting. He’s had moments of confusion due to the hypos but is generally very with it when lucid.
We live 3 hours away and there’s no other family (we’re taking steps to address this but that’s a separate issue). He can’t come to stay with us due to his dialysis. I can work from home (my husband can’t) so have stayed with him for a few days to try to get him back on an even keel but have commitments at home that mean I have to come back after a couple of days and even with really close supervision, it’s still happening.
The diabetes team have now told us to tolerate the highs to help avoid the lows so he’s not having any corrective doses of insulin after his evening meal. I’m writing this at 5am as I’ve been up with him four times and have now given up on sleep. Overnight (when his blood sugar usually drops very low) he hasn’t dipped below 27. It hasn’t changed since 3pm yesterday despite 5 units of Novorapid at 1pm with a small lunch and 8 units at 6pm when he again had a small meal. These amounts are what he has now been told to take and are dependent on his pre-meal blood sugar level. He’s drinking as much as his dialysis team allow him.
There has to be something underlying causing this but the hospital just don’t seem to want to know. They say they’ve run tests and there is nothing. We’re at a loss as to what to try next. Does anybody have any thoughts / experience of something similar please?