JontyW
Active Member
- Relationship to Diabetes
- Type 1
I have had Type 1 diabetes for 43 years and have been generally well controlled with an average HbA1c of < 7.5%, and as a consequence have experienced no complications. My good control has been achieved by generally having the same amount of carbohydrate for the same meal each day (as was the technique needed in the days before MDI basal/bolus) and dosing based on previously achieved blood glucose results. I eat a lowish-carb diet of about 110 - 130g per day.
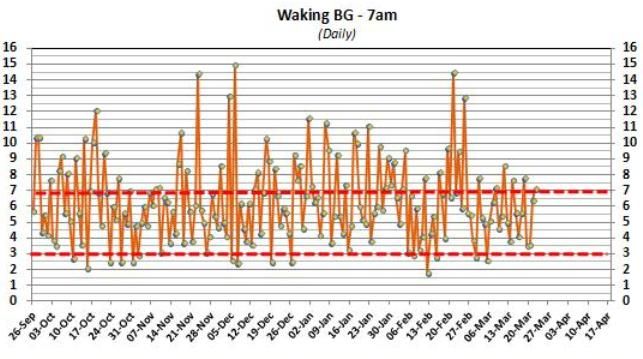
More recently I have started reading some diabetes websites to get a better understanding of how to manage my MDI basal/bolus regime since I had been provided limited information on how to optimise this. From these websites I found out about carb counting and the concept of Insulin-Carb Ratios (ICR). So for the last 8 months I have been recording on a daily basis, in a detailed Excel spreadsheet that I have developed myself, all the required data (BG before each meal, carbs, basal each day and bolus each meal, plus comments as needed) to get a better understanding on what might be changing.
Note: I have a degree in Physics so am used to conducting controlled experiments and recording/plotting/reviewing the data. I think this background has indeed helped in achieving my good control so far.
In the spreadsheet I have developed a traffic light system (green - in target,amber - just out, red - out of target) which helps to highlight ongoing changes. In addition I have multiple graphs displaying the daily, 3-day or 5-day average values for all the key metrics. So you can see I have an extremely comprehensive recording and reviewing system. This also predicts the carb bolus required for next meal based on previous BG results (prev day and 3-day ave) and ICR used, and also adds on any correction dose. So carb bolus is always calculated very accurately using the IC Ratio.
Now to my main question: one piece of information that I found from my web searches was about the IC Ratio, and in particular how it can change throughout the day, so each meal (breakfast, lunch and dinner) has a different ratio. I previously had no idea about this concept, and the fact the difference can be so large!
Here are my ratios: Insulin units per 10g CHO
Breakfast:- 11 (40g needs 44u)
Lunch:- 3 (40g needs 12u)
Dinner:- 4 (40g needs 16u)
Questions I would like you to answer:-
1. Why is my breakfast ICR so much higher than the other meals? Bfast -> Dinner = 11 -> 4 (2.8 times MORE bolus needed at Bfast).
2. What is the 'mechanism' in the body that is changing in the first part of the day to require so much more bolus?
2. Up until mid-Nov 2012 the breakfast ICR was about 5, then for no apparent reason it escalated to ~ 10, and has been about this level ever since. See attached screenshot "ICR - JontyW" which shows the 5-day average graph. The Bfast ICR had to be increased to overcome high BG levels pre-lunch. Note that the Dinner ICR has remained constant in the range 3.5 to 4.5, with no dramatic change.
Note: my basal is 12u of Lantus taken in morning and unchanged during the above period.
I would welcome anyone's ideas on this subject .. thanks.
Jonty
More recently I have started reading some diabetes websites to get a better understanding of how to manage my MDI basal/bolus regime since I had been provided limited information on how to optimise this. From these websites I found out about carb counting and the concept of Insulin-Carb Ratios (ICR). So for the last 8 months I have been recording on a daily basis, in a detailed Excel spreadsheet that I have developed myself, all the required data (BG before each meal, carbs, basal each day and bolus each meal, plus comments as needed) to get a better understanding on what might be changing.
Note: I have a degree in Physics so am used to conducting controlled experiments and recording/plotting/reviewing the data. I think this background has indeed helped in achieving my good control so far.
In the spreadsheet I have developed a traffic light system (green - in target,amber - just out, red - out of target) which helps to highlight ongoing changes. In addition I have multiple graphs displaying the daily, 3-day or 5-day average values for all the key metrics. So you can see I have an extremely comprehensive recording and reviewing system. This also predicts the carb bolus required for next meal based on previous BG results (prev day and 3-day ave) and ICR used, and also adds on any correction dose. So carb bolus is always calculated very accurately using the IC Ratio.
Now to my main question: one piece of information that I found from my web searches was about the IC Ratio, and in particular how it can change throughout the day, so each meal (breakfast, lunch and dinner) has a different ratio. I previously had no idea about this concept, and the fact the difference can be so large!
Here are my ratios: Insulin units per 10g CHO
Breakfast:- 11 (40g needs 44u)
Lunch:- 3 (40g needs 12u)
Dinner:- 4 (40g needs 16u)
Questions I would like you to answer:-
1. Why is my breakfast ICR so much higher than the other meals? Bfast -> Dinner = 11 -> 4 (2.8 times MORE bolus needed at Bfast).
2. What is the 'mechanism' in the body that is changing in the first part of the day to require so much more bolus?
2. Up until mid-Nov 2012 the breakfast ICR was about 5, then for no apparent reason it escalated to ~ 10, and has been about this level ever since. See attached screenshot "ICR - JontyW" which shows the 5-day average graph. The Bfast ICR had to be increased to overcome high BG levels pre-lunch. Note that the Dinner ICR has remained constant in the range 3.5 to 4.5, with no dramatic change.
Note: my basal is 12u of Lantus taken in morning and unchanged during the above period.
I would welcome anyone's ideas on this subject .. thanks.
Jonty
Last edited:
 .. hypo time :-(
.. hypo time :-(