-
Please Remember: Members are only permitted to share their own experiences. Members are not qualified to give medical advice. Additionally, everyone manages their health differently. Please be respectful of other people's opinions about their own diabetes management.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Why does ny blood sugar go up overnight ?
- Thread starter NicF
- Start date
Leadinglights
Well-Known Member
- Relationship to Diabetes
- Type 2
- Pronouns
- She/Her
Dawn Phenomenon or Foot on the Floor syndrome depending on when it happens, caused by the liver being super helpful in releasing glucose in the absence of food to give you energy for your organs to function and for the early activity, getting up etc.I'm a bit confused, I always thought your blood sugar goes down overnight, but mine seems to be fairly stable and dips slightly around 3am and then goes up ?
Proud to be erratic
Well-Known Member
- Relationship to Diabetes
- Type 3c
- Pronouns
- He/Him
Hello @NicF, welcome to the forum. Also welcome to the "visibility" that CGM can bring to things going on inside you. To help me get some perspective about your question, could I ask how long have you had your diagnosis of T2? When did you decide to improve your monitoring and were you using finger prick testing before you got your Libre?
During the night our brains are, apparently, at their most active doing our internal housework! Who knew .... I certainly didn't! To keep the brain functioning it needs glucose and during fasting hours that glucose comes from the liver's glucose store. Almost a digression, but significantly our brain doesn't need insulin to enable the transfer of glucose from blood to brain. Anyway there is a deceptively large amount of metabolic and other activity going on overnight, while we are fasting and sleeping.
During the night our brains are, apparently, at their most active doing our internal housework! Who knew .... I certainly didn't! To keep the brain functioning it needs glucose and during fasting hours that glucose comes from the liver's glucose store. Almost a digression, but significantly our brain doesn't need insulin to enable the transfer of glucose from blood to brain. Anyway there is a deceptively large amount of metabolic and other activity going on overnight, while we are fasting and sleeping.
The Dawn Phenomenon. A release of energy just before dawn to set you for morning. Very useful when we had to get up and chase Woolly Mammoth for breakfast, not so useful now. Various methods suggested to trick it e.g. a small amount of long lasting carb at bedtime.I'm a bit confused, I always thought your blood sugar goes down overnight, but mine seems to be fairly stable and dips slightly around 3am and then goes up ?
The only way i have found to avoid Dawn Phenomenon is intensive exercise the day before.
During exercise, our body is more efficient at using insulin and our liver dumps glucose to give us the energy to maintain the "mammoth chasing" (or whatever else you are running to/from).
Therefore, there is less glucose available for the liver the next day.
During exercise, our body is more efficient at using insulin and our liver dumps glucose to give us the energy to maintain the "mammoth chasing" (or whatever else you are running to/from).
Therefore, there is less glucose available for the liver the next day.
rebrascora
Well-Known Member
- Relationship to Diabetes
- Type 1
- Pronouns
- She/Her
I too was going to suggest exercise to help reduce or eliminate DP, the evening before works well for me.
harbottle
Well-Known Member
- Relationship to Diabetes
- Type 2
The only way i have found to avoid Dawn Phenomenon is intensive exercise the day before.
During exercise, our body is more efficient at using insulin and our liver dumps glucose to give us the energy to maintain the "mammoth chasing" (or whatever else you are running to/from).
Therefore, there is less glucose available for the liver the next day.
Not sure it’s anything to do with ‘less glucose available’
The body always makes sure it has enough glucose. If muscle/liver stores are depleted it will make it via a different pathway. DP is associated with an increase of hepatic synthesis from other sources, via gluconeogenesis, and increased insulin resistance due to hormones. I suspect that the exercise makes you more insulin sensitive for a period of time so your muscles slurp up the glucose made by the liver more effectively by counteracting the hormones.
dannybgoode
Well-Known Member
- Relationship to Diabetes
- Type 2
Sorry, i don't understand some of the words you use. It has always been explained to me in much simpler terms.Not sure it’s anything to do with ‘less glucose available’
The body always makes sure it has enough glucose. If muscle/liver stores are depleted it will make it via a different pathway. DP is associated with an increase of hepatic synthesis from other sources, via gluconeogenesis, and increased insulin resistance due to hormones. I suspect that the exercise makes you more insulin sensitive for a period of time so your muscles slurp up the glucose made by the liver more effectively by counteracting the hormones.
I know it is recommended that people who treat their diabetes with basal - bolus regime reduce their basal insulin for up to 48 hours after intensive exercise. I have found this is cumulative - on a 10 day walking holiday, I needed to reduce my basal each day to avoid hypos because my liver dripped/dumped less glucose.
rebrascora
Well-Known Member
- Relationship to Diabetes
- Type 1
- Pronouns
- She/Her
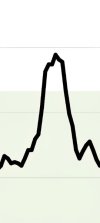
I used to need to prebolus 75 mins in advance of breakfast with NR to prevent regularly spiking like that up to 15 and then back down to 5 and the drop back down was not overly pleasant. It was one of the main reasons I changed to Fiasp, but still need 45 mins with that most mornings. For me the key thing is to inject it before I get out of bed, to prevent the rise, but obviously that doesn't work with everyone's routine, especially if you go for a run or walk the dog before breakfast, although those activities might negate the spike a bit. Definitely not recommending running or walking with bolus insulin on board though.I find exercise mates zero difference to the vertical upward line which is my DP.
This is a pretty standard representation even with 8.5U of NR 45mins before I have a low carb breakfast even with a good run the night before...
dannybgoode
Well-Known Member
- Relationship to Diabetes
- Type 2
I've left it longer before eating. Didn't make much of a difference. I don't have time in the morning to get up over an hour before I'm due to eat.I used to need to prebolus 75 mins in advance of breakfast with NR to prevent regularly spiking like that up to 15 and then back down to 5 and the drop back down was not overly pleasant. It was one of the main reasons I changed to Fiasp, but still need 45 mins with that most mornings. For me the key thing is to inject it before I get out of bed, to prevent the rise, but obviously that doesn't work with everyone's routine, especially if you go for a run or walk the dog before breakfast, although those activities might negate the spike a bit. Definitely not recommending running or walking with bolus insulin on board though.
I just live with the spike, doesn't really matter much. I'm not going to mess about trying to stay 100% TIR. 80%+ is my target and I'm easily within that.
NR works great otherwise so I'll stick to what I know for now 🙂
I used to need to prebolus 75 mins in advance of breakfast with NR to prevent regularly spiking like that up to 15 and then back down to 5 and the drop back down was not overly pleasant. It was one of the main reasons I changed to Fiasp, but still need 45 mins with that most mornings. For me the key thing is to inject it before I get out of bed, to prevent the rise, but obviously that doesn't work with everyone's routine, especially if you go for a run or walk the dog before breakfast, although those activities might negate the spike a bit. Definitely not recommending running or walking with bolus insulin on board though.
I had this problem. Took high dose of insulin to get my sugar down and ended up with a hypo before lunch. My diabetic nurse recommended two eggs I.e an omelette for breakfast and no carbohydrate with a low dose of insulin. This has stabilised my sugar levels and now I am never hungry before lunch
rebrascora
Well-Known Member
- Relationship to Diabetes
- Type 1
- Pronouns
- She/Her
@Andricles I have it sorted now thanks and rarely go above 8 and I like my yoghurt, berries and seeds for breakfast. Injecting my breakfast bolus insulin (plus 2 extra units to cover FOTF) before I even sit up in bed keeps it from going any higher and then I just wait until it starts to come down or I can see the insulin is active and then I eat. Not sure I could face eggs for breakfast every morning but nice as an occasional treat.
dannybgoode
Well-Known Member
- Relationship to Diabetes
- Type 2
I would note for me also that my BG goes from 6-7 to 9-10+ with 8.5U of NR on board and not eating anything! it really does rocket up with no input from me 
Hi, I've been type 2 for over 20 years, both my nan and my mum were diabetic so they were watching me early, tried to control it with diet, then tablets but gradually the control has been getting worse. I was really bad at doing the finger pricks but generally when I did it it was OK.Hello @NicF, welcome to the forum. Also welcome to the "visibility" that CGM can bring to things going on inside you. To help me get some perspective about your question, could I ask how long have you had your diagnosis of T2? When did you decide to improve your monitoring and were you using finger prick testing before you got your Libre?
During the night our brains are, apparently, at their most active doing our internal housework! Who knew .... I certainly didn't! To keep the brain functioning it needs glucose and during fasting hours that glucose comes from the liver's glucose store. Almost a digression, but significantly our brain doesn't need insulin to enable the transfer of glucose from blood to brain. Anyway there is a deceptively large amount of metabolic and other activity going on overnight, while we are fasting and sleeping.
I've been on insulin for about 5 years as well as tablets. In December they added monjaro and gave me a CGM which has been a revelation in itself !
Thanks for your support.
goodybags
Well-Known Member
- Relationship to Diabetes
- Type 2
Like you @NicF I also needed insulin on top of tablets (some of us T2’s do) then both Mounjaro and a CGM were prescribed to me (8 months ago) to now give me a decent control, how you getting on with MJ ?Hi, I've been type 2 for over 20 years, both my nan and my mum were diabetic so they were watching me early, tried to control it with diet, then tablets but gradually the control has been getting worse. I was really bad at doing the finger pricks but generally when I did it it was OK.
I've been on insulin for about 5 years as well as tablets. In December they added monjaro and gave me a CGM which has been a revelation in itself !
Thanks for your support.
Hi Goodybags, tbh I haven't felt great on MJ, feel quite dizzy and just 'not right'.Like you @NicF I also needed insulin on top of tablets (some of us T2’s do) then both Mounjaro and a CGM were prescribed to me (8 months ago) to now give me a decent control, how you getting on with MJ ?
My HBA1C was 68 before MJ, got a blood test in a few weeks so will be interesting to see if it's come down.
My diabetic nurse told me to reduce my insulin from 30 to 26 but my levels really spiked so after christmas I put it back up and have managed to reduce it to 28.
I think they will put the MJ up to 7.5 though.
No other side effects apart from a little nausea.
How about you ?
Proud to be erratic
Well-Known Member
- Relationship to Diabetes
- Type 3c
- Pronouns
- He/Him
In principle, regardless of sex or age, sleep deprivation is not a good thing. In recent years there have been various studies across the western world about the physical and psychological effects, some not as conclusive as others. The NHS offers some pointers:Thanks to everyone for your comments, I'd heard of DP but not foot on the floor, just wondering if being a woman of a certain age and getting up several times a night for a wee or to walk about due to restless legs has any impact .
Sleep problems - Every Mind Matters
Learn about sleep problems, including what it means to be sleep deprived or have insomnia. Plus find out how sleep hygiene can help if you are struggling to sleep.
 www.nhs.uk
www.nhs.uk
However, I'm not convinced that getting "sleep tips" sent to one's inbox is such a great idea. It takes a lot of self control to not turn to a sleep interfering screen, when already awake in the small hours.
Needing a wee several times a night is clearly unhelpful as well, or are the restless legs the main cause of your interrupted sleep?
What insulin(s), including any letters or numbers on the packaging and with what typical dose size? Is this a background basal, once or twice a day? Or a combined basal/bolus insulin, usually twice daily? Or possibly even 2 different insulins: basal (once or twice daily) and a bolus insulin with each meal - ie Multiple Daily Injections (MDI).I've been on insulin for about 5 years as well as tablets. In December they added monjaro and gave me a CGM which has been a revelation in itself !
Delighted that someone has had the vision to recognise that a CGM can be appropriate for you. Not all T2s are so fortunate.
- Relationship to Diabetes
- Type 1
- Pronouns
- He/Him
Thanks to everyone for your comments, I'd heard of DP but not foot on the floor, just wondering if being a woman of a certain age and getting up several times a night for a wee or to walk about due to restless legs has any impact .
I think FOTF is a bit of a forum-ism. Most Drs who have heard of Dawn Phenomenon just call it that I think.
Some of us on the forum noticed though that our trigger is not a specific overnight time period, it only happens whenever we get out of bed.
So my BG will just pootle along pretty much completely level, if my basal insulin is set right, from say 3am to 6am, or 7am or 8am or even 9am if I’m on holiday, but there’s a noticeable ‘bump’ soon after I get up, whenever that is.