Joanneclairebarnes
Member
- Relationship to Diabetes
- Type 1
Any thoughts….I was initially diagnosed Type 1 aged 19. Well controlled and didn’t see a consultant regularly until became pregnant at 30, due to low insulin requirements at time (thought definitely needing it) i was test for MODY, negative. Also had cpeptide test which indicated insulin production.
i have since then been labelled as "Likely Type 2". Tried coming off insulin and just having metformin, empagliflozin and gliclazide but this didn't control my glucose at all so back on insulin. I take 10 lantus, and 8-10 novorapid with evening meal( plus minimal novorapid at lunch but tend to eat low carb)
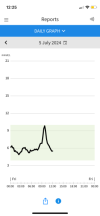
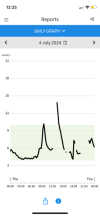
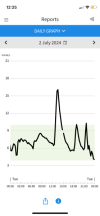
Most recently, consultant said that although i dont fit Type2 profile, test have proven I'm not type 1. Managed to get them to repeat c-peptide. Results attached. There is note saying "low for insulin level"
Im going to speak to them asap of course but any thoughts or ideas?! I was most recently told its either an unknown type of diabetes, or an underlying condition causing the symptoms. I just hate the not knowing!!
i have since then been labelled as "Likely Type 2". Tried coming off insulin and just having metformin, empagliflozin and gliclazide but this didn't control my glucose at all so back on insulin. I take 10 lantus, and 8-10 novorapid with evening meal( plus minimal novorapid at lunch but tend to eat low carb)
Most recently, consultant said that although i dont fit Type2 profile, test have proven I'm not type 1. Managed to get them to repeat c-peptide. Results attached. There is note saying "low for insulin level"
Im going to speak to them asap of course but any thoughts or ideas?! I was most recently told its either an unknown type of diabetes, or an underlying condition causing the symptoms. I just hate the not knowing!!