A few weeks back I posted about my recent unexpected/difficult-to-manage highs/lows, after 40 years of being well-controlled as an insulin dependent type 1. Finally got to see a consultant today who has recommended an insulin pump. I recognise we're all different but I'd be grateful for comments from those who've had a similar pathway, whether the change improved control, and general pros/cons from actual experience. Many thanks for the responses.
-
Please Remember: Members are only permitted to share their own experiences. Members are not qualified to give medical advice. Additionally, everyone manages their health differently. Please be respectful of other people's opinions about their own diabetes management.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Move from injections to pump...any thoughts from those who have done same
- Thread starter ChrisLG
- Start date
- Status
- This thread is now closed. Please contact Anna DUK, Ieva DUK or everydayupsanddowns if you would like it re-opened.
Hi Chris.
My name is Elaine. I’ve had the same problem. I am now on a pump. I started my Omnipod DASH in September 2024. To be honest I was offered many different pumps but the most important thing for me was the pump being tubeless.
The pros for me.
small device
Tubeless
Auto cannula insertion
Easy to apply
72 hours in use
No injections
PDM is easy to navigate
Warning alarms
Waterproof up to 1 hour
Cons for me.
I don’t really have any.
I’ve had 2 pods that didn’t beep when filling with the insulin but I carried on with the priming process and used them for the full 3 days.
On the whole I love it. So much nicer when out & about. No more leaving your friends to go and inject in a toilet.
You still have to work out your carbs and check your BG but the PDM will work out your insulin dose.
Just research all the pumps that are offered.
The Omnipod group of pumps are all tubeless and that was for me and the only pump that I have used.
I hope that you consider a pump as it’s helping with the highs and lows in quite a short time.
Good luck Chris.
My name is Elaine. I’ve had the same problem. I am now on a pump. I started my Omnipod DASH in September 2024. To be honest I was offered many different pumps but the most important thing for me was the pump being tubeless.
The pros for me.
small device
Tubeless
Auto cannula insertion
Easy to apply
72 hours in use
No injections
PDM is easy to navigate
Warning alarms
Waterproof up to 1 hour
Cons for me.
I don’t really have any.
I’ve had 2 pods that didn’t beep when filling with the insulin but I carried on with the priming process and used them for the full 3 days.
On the whole I love it. So much nicer when out & about. No more leaving your friends to go and inject in a toilet.
You still have to work out your carbs and check your BG but the PDM will work out your insulin dose.
Just research all the pumps that are offered.
The Omnipod group of pumps are all tubeless and that was for me and the only pump that I have used.
I hope that you consider a pump as it’s helping with the highs and lows in quite a short time.
Good luck Chris.
Bruce Stephens
Well-Known Member
- Relationship to Diabetes
- Type 1
Depending on your clothing, there's usually no need to do that! (I can imagine sometimes clothing limits your options too much.)No more leaving your friends to go and inject in a toilet.
Ivostas66
Well-Known Member
- Relationship to Diabetes
- Type 1
I was on the Omnipod Dash from Feb this year. My control when injecting was considered 'excellent' by my consultant and only improved on the pump. I have just moved onto the Omnipod 5 system and that automated system is taking more getting used to. Like @Eps57 it was the tubeless nature of the Omnipod system I found appealing. I have had the odd screamer when swimming - although waterproof and suitable for swimming for up to an hour, some pods have shut down and they set off a loud alarm.
When you attend the orientation session make sure you ask them about the suitability of your insulin for the pump. Some can cause 'tunneling' which is where insulin can seep out from the canula - this tends to be thinner faster acting insulins like Fiasp and usually when a larger dose is being pumped. I had a period of two weeks with higher than usual levels. I noticed the pod was wet with insulin when removed. Extending larger doses of insulin over 30 minutes or so solved the problem. Some insulin can also crystalise in certain pumps, so again, worth checking.
When you attend the orientation session make sure you ask them about the suitability of your insulin for the pump. Some can cause 'tunneling' which is where insulin can seep out from the canula - this tends to be thinner faster acting insulins like Fiasp and usually when a larger dose is being pumped. I had a period of two weeks with higher than usual levels. I noticed the pod was wet with insulin when removed. Extending larger doses of insulin over 30 minutes or so solved the problem. Some insulin can also crystalise in certain pumps, so again, worth checking.
nonethewiser
Well-Known Member
- Relationship to Diabetes
- Type 1
Transition from pens went smoothly, more smoothly than expected if honest.
Only pro's have no negatives to mention, better bg control more options to bolus for meals & much flatter bg levels throughout night, that's just a few there's many more advantages of a pump over mdi.
Only pro's have no negatives to mention, better bg control more options to bolus for meals & much flatter bg levels throughout night, that's just a few there's many more advantages of a pump over mdi.
mashedupmatt
Moderator
- Relationship to Diabetes
- Type 1
Can you put me in touch with your consultant please (I've never even seen one!) as I've been trying to get a pump (with no success!!) - only joking (well not really!) - I've seen very few (if any) Negative comments about being put on a pump as opposed to MDI - I hope you get on well with it (if you decide to take up the offer) and let us all know how you get on
Inka
Well-Known Member
- Relationship to Diabetes
- Type 1
Changing to a pump smoothed out my control because the basal matched my needs, which vary a lot over 24hrs, whereas no basal insulin could. I’ve now used a pump for almost 21 years. I’ve always used tubed pumps because I prefer them and find them more flexible. My current pump is a Dana i, but I’ve had a few different ones over the years.
The major pro of a pump is the ability to fine-tune your basal. This is by far the best thing IMO. Other pros are not having to inject, but that’s more for convenience (I can use my phone to bolus on my pump); being able to have more closely tailored bolus doses, eg 5.35 units and not having to round up or down.
The negatives are the increased ‘stuff’ you need (sets, cannulas, reservoirs, etc); the increased risk of DKA; and the increased risk of site infections, which can be very unpleasant.
My advice @ChrisLG is to focus on what’s best for you as an individual. Find out exactly why the consultant thinks a pump will suit you (eg is it to do with absorption, extended boluses, etc etc) and think whether you’d like to have a pump. If you’re happy on MDI, you don’t have to. Each has pros and cons, and MDI is simpler. Then find out what pumps would be on offer to you and start researching them - very thoroughly! There is no ‘best’ pump, only the best pump for you.
The major pro of a pump is the ability to fine-tune your basal. This is by far the best thing IMO. Other pros are not having to inject, but that’s more for convenience (I can use my phone to bolus on my pump); being able to have more closely tailored bolus doses, eg 5.35 units and not having to round up or down.
The negatives are the increased ‘stuff’ you need (sets, cannulas, reservoirs, etc); the increased risk of DKA; and the increased risk of site infections, which can be very unpleasant.
My advice @ChrisLG is to focus on what’s best for you as an individual. Find out exactly why the consultant thinks a pump will suit you (eg is it to do with absorption, extended boluses, etc etc) and think whether you’d like to have a pump. If you’re happy on MDI, you don’t have to. Each has pros and cons, and MDI is simpler. Then find out what pumps would be on offer to you and start researching them - very thoroughly! There is no ‘best’ pump, only the best pump for you.
Hi ElaineHi Chris.
My name is Elaine. I’ve had the same problem. I am now on a pump. I started my Omnipod DASH in September 2024. To be honest I was offered many different pumps but the most important thing for me was the pump being tubeless.
The pros for me.
small device
Tubeless
Auto cannula insertion
Easy to apply
72 hours in use
No injections
PDM is easy to navigate
Warning alarms
Waterproof up to 1 hour
Cons for me.
I don’t really have any.
I’ve had 2 pods that didn’t beep when filling with the insulin but I carried on with the priming process and used them for the full 3 days.
On the whole I love it. So much nicer when out & about. No more leaving your friends to go and inject in a toilet.
You still have to work out your carbs and check your BG but the PDM will work out your insulin dose.
Just research all the pumps that are offered.
The Omnipod group of pumps are all tubeless and that was for me and the only pump that I have used.
I hope that you consider a pump as it’s helping with the highs and lows in quite a short time.
Good luck Chris.
Much appreciate your comments. Thank you. Chris
Hi Inka, Many thanks for all the useful info. You asked why the consultant advised going for a pump: for the last 2 months, BG levels have been bouncing up and down (previously they hadn't) in ways that were unpredictable and which made my responses (either bolus or carbs) also unpredictable. This is in part due to delayed GI absorption and the consultant considered all of this was well suited to a pump... so very much for improved BG control and nothing to do with actual insulin administration.Changing to a pump smoothed out my control because the basal matched my needs, which vary a lot over 24hrs, whereas no basal insulin could. I’ve now used a pump for almost 21 years. I’ve always used tubed pumps because I prefer them and find them more flexible. My current pump is a Dana i, but I’ve had a few different ones over the years.
The major pro of a pump is the ability to fine-tune your basal. This is by far the best thing IMO. Other pros are not having to inject, but that’s more for convenience (I can use my phone to bolus on my pump); being able to have more closely tailored bolus doses, eg 5.35 units and not having to round up or down.
The negatives are the increased ‘stuff’ you need (sets, cannulas, reservoirs, etc); the increased risk of DKA; and the increased risk of site infections, which can be very unpleasant.
My advice @ChrisLG is to focus on what’s best for you as an individual. Find out exactly why the consultant thinks a pump will suit you (eg is it to do with absorption, extended boluses, etc etc) and think whether you’d like to have a pump. If you’re happy on MDI, you don’t have to. Each has pros and cons, and MDI is simpler. Then find out what pumps would be on offer to you and start researching them - very thoroughly! There is no ‘best’ pump, only the best pump for you.
Yes.. I am researching the pumps which this site says are offered by the NHS. If anyone knows of a comparative pros/cons table, then I'd be grateful for the link. Thanks Chris
Thanks for this. Yes, it was a put of a push to see the consultant. In fact last November I had one of these episodes where I couldn't get the low BG to respond to a lot of fast-acting glucose and ended up in hospital in Hong Kong...where I did get to see an endocrinology consultant, and that was the first time in about 15 years. I forwarded her discharge letter which was addressed "dear UK consultant - please see this patient" to my GP and pushed my diabetic nurse for a consult on the basis that I needed help and if I didn't get any I was likely to end up in A&E...which is precisely what happened the other week (although for high BG which was non-responsive to insulin).Can you put me in touch with your consultant please (I've never even seen one!) as I've been trying to get a pump (with no success!!) - only joking (well not really!) - I've seen very few (if any) Negative comments about being put on a pump as opposed to MDI - I hope you get on well with it (if you decide to take up the offer) and let us all know how you get on
Many thanks for your response. All good to hear.Transition from pens went smoothly, more smoothly than expected if honest.
Only pro's have no negatives to mention, better bg control more options to bolus for meals & much flatter bg levels throughout night, that's just a few there's many more advantages of a pump over mdi.
mashedupmatt
Moderator
- Relationship to Diabetes
- Type 1
See attached - this is a comparison of pumps used for HCL that are NHS approved - Might be a bit small to read - go to https://www.diabetesspecialistnurseforumuk.co.uk/hcp-resources and look at the "Insulin Pumps & Technology section to download the pdf versionHi Inka, Many thanks for all the useful info. You asked why the consultant advised going for a pump: for the last 2 months, BG levels have been bouncing up and down (previously they hadn't) in ways that were unpredictable and which made my responses (either bolus or carbs) also unpredictable. This is in part due to delayed GI absorption and the consultant considered all of this was well suited to a pump... so very much for improved BG control and nothing to do with actual insulin administration.
Yes.. I am researching the pumps which this site says are offered by the NHS. If anyone knows of a comparative pros/cons table, then I'd be grateful for the link. Thanks Chris

Inka
Well-Known Member
- Relationship to Diabetes
- Type 1
This is in part due to delayed GI absorption and the consultant considered all of this was well suited to a pump... so very much for improved BG control and nothing to do with actual insulin administration.
@ChrisLG A pump could well help GI problems as they have the ability to do different boluses, eg an extended bolus, that is released over a longer period of time. So, yes, it would be to do with insulin administration. A pump is just another insulin delivery system 🙂
The best pump comparison chart is the one you’re about to make yourself! More isn’t necessarily better, and different people have different needs. Get the list of available pumps, reduce that down to two or three, then start researching and identifying what you want.
@ChrisLG A pump could well help GI problems as they have the ability to do different boluses, eg an extended bolus, that is released over a longer period of time. So, yes, it would be to do with insulin administration. A pump is just another insulin delivery system 🙂
The best pump comparison chart is the one you’re about to make yourself! More isn’t necessarily better, and different people have different needs. Get the list of available pumps, reduce that down to two or three, then start researching and identifying what you want.
I started pumping after about 12 years of mdi.
My main motivation was to reduce hypos while exercising which it has certainly done as well as allowed me to keep closer eye on my BG and react more easily.
I have now been pumping for 8 years and the best management I have had is in recent years when I have learned more about how my body benefits from different boluses (do I have it all up front, 50% up front and the rest over the next 3 hours, none upfront and all of it spread over the next 90 minutes, etc.) - the answer is typically, "it depends, ..."
I have also found it easier when working with my phone on my desk showing my CGM readings and allowing me to give myself a little bolus nudge or suspend my basal before I heard downhill too fast.
Just like there are IT people who think Apple computers are the bees knees and as many who think Windows is better (and then another bunch who can't believe the world does not use Linux all the time), there are tubeless pumping fans and tubed pumping fans. I have used both and see pros and cons with both. My preference is tubeless but if there was a tubed pump with all the features I want, I would not ignore it. What I am saying is try not to be swayed by Omnipod evangelists or T-Slim superfans - the best pump for you is the one you can get and the one that satisfies your needs.
For example, today, one of my biggest requirements would be to be able to manage my pump from my phone. But many people hate being tied to theirs and would prefer controls on their pump.
Whatever you decide, ignore all comparison charts until you know what pumps your clinic offers. It is a waste of time and emotions setting your heart on a pump that you cannot get. For many years, my clinic only offered Medtronic and, still consider Omnipod too expensive. Thankfully, there are other tubeless pumps. And any pump your clinic offers will be good.
My main motivation was to reduce hypos while exercising which it has certainly done as well as allowed me to keep closer eye on my BG and react more easily.
I have now been pumping for 8 years and the best management I have had is in recent years when I have learned more about how my body benefits from different boluses (do I have it all up front, 50% up front and the rest over the next 3 hours, none upfront and all of it spread over the next 90 minutes, etc.) - the answer is typically, "it depends, ..."
I have also found it easier when working with my phone on my desk showing my CGM readings and allowing me to give myself a little bolus nudge or suspend my basal before I heard downhill too fast.
Just like there are IT people who think Apple computers are the bees knees and as many who think Windows is better (and then another bunch who can't believe the world does not use Linux all the time), there are tubeless pumping fans and tubed pumping fans. I have used both and see pros and cons with both. My preference is tubeless but if there was a tubed pump with all the features I want, I would not ignore it. What I am saying is try not to be swayed by Omnipod evangelists or T-Slim superfans - the best pump for you is the one you can get and the one that satisfies your needs.
For example, today, one of my biggest requirements would be to be able to manage my pump from my phone. But many people hate being tied to theirs and would prefer controls on their pump.
Whatever you decide, ignore all comparison charts until you know what pumps your clinic offers. It is a waste of time and emotions setting your heart on a pump that you cannot get. For many years, my clinic only offered Medtronic and, still consider Omnipod too expensive. Thankfully, there are other tubeless pumps. And any pump your clinic offers will be good.
Great. Thank youSee attached - this is a comparison of pumps used for HCL that are NHS approved - Might be a bit small to read - go to https://www.diabetesspecialistnurseforumuk.co.uk/hcp-resources and look at the "Insulin Pumps & Technology section to download the pdf version
View attachment 32402
Many thanks for this helpful info.I started pumping after about 12 years of mdi.
My main motivation was to reduce hypos while exercising which it has certainly done as well as allowed me to keep closer eye on my BG and react more easily.
I have now been pumping for 8 years and the best management I have had is in recent years when I have learned more about how my body benefits from different boluses (do I have it all up front, 50% up front and the rest over the next 3 hours, none upfront and all of it spread over the next 90 minutes, etc.) - the answer is typically, "it depends, ..."
I have also found it easier when working with my phone on my desk showing my CGM readings and allowing me to give myself a little bolus nudge or suspend my basal before I heard downhill too fast.
Just like there are IT people who think Apple computers are the bees knees and as many who think Windows is better (and then another bunch who can't believe the world does not use Linux all the time), there are tubeless pumping fans and tubed pumping fans. I have used both and see pros and cons with both. My preference is tubeless but if there was a tubed pump with all the features I want, I would not ignore it. What I am saying is try not to be swayed by Omnipod evangelists or T-Slim superfans - the best pump for you is the one you can get and the one that satisfies your needs.
For example, today, one of my biggest requirements would be to be able to manage my pump from my phone. But many people hate being tied to theirs and would prefer controls on their pump.
Whatever you decide, ignore all comparison charts until you know what pumps your clinic offers. It is a waste of time and emotions setting your heart on a pump that you cannot get. For many years, my clinic only offered Medtronic and, still consider Omnipod too expensive. Thankfully, there are other tubeless pumps. And any pump your clinic offers will be good.
- Relationship to Diabetes
- Type 1
- Pronouns
- He/Him
This is in part due to delayed GI absorption and the consultant considered all of this was well suited to a pump... so very much for improved BG control and nothing to do with actual insulin administration.
By GI, are you talking about Gastro Intestinal? or Glycaemic Index? Just wondering if you may have a degree of gastroparesis (delayed stomach emptying) which is making things more erratic for you?
One member here, @AJLang has had great success with using the flexibility of a pump to help improve her management with gastroparesis (which is notoriously difficult).
It was a long time ago now, and technology has moved on a LOT, but these were my thoughts when I’d only been on a pump for a few short months.

Face-off: MDI vs Pump
Because no two days with type 1 diabetes are the same. Except when they are. The ups and downs of life with T1D.
Very good point and my apologies...I meant Gastro Intestina, gastroparesis is certainly on the radar and I'm waiting for both barium swallow and gastro emptying appointments. Typical episode is a bolus followed by a meal but a delay in carb absorption leading to lowered BG which can be non-responsive to attempts to elevate. Great advice from this forum means I now take 50% of bolus as I start to eat and the balance when absence of symptoms indicates there won't be an episode. It has lead to a BG which for 50% of the time is now between 10 and 14 so I am very much hoping the pump will bring me back long-term into range.By GI, are you talking about Gastro Intestinal? or Glycaemic Index? Just wondering if you may have a degree of gastroparesis (delayed stomach emptying) which is making things more erratic for you?
One member here, @AJLang has had great success with using the flexibility of a pump to help improve her management with gastroparesis (which is notoriously difficult).
It was a long time ago now, and technology has moved on a LOT, but these were my thoughts when I’d only been on a pump for a few short months.
Face-off: MDI vs Pump
Because no two days with type 1 diabetes are the same. Except when they are. The ups and downs of life with T1D.www.everydayupsanddowns.co.uk
H @ChrisLG
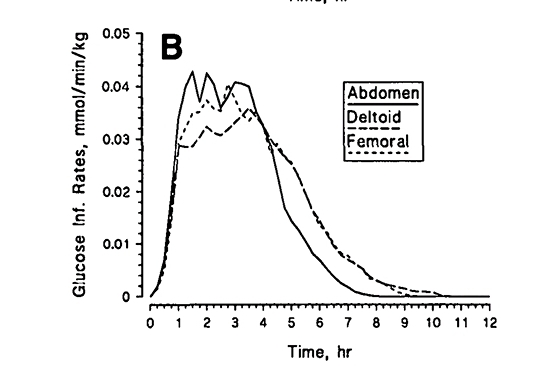
As you were writing about absorption issues, I thought of you as I read this
 www.diabettech.com
www.diabettech.com
As the article mentions, the sample size was small but it could be interesting wrt where to inject (yes, the article talks about pumps but absorption issues maybe the same with injections) and the different insulin profiles.
As you were writing about absorption issues, I thought of you as I read this
Location, location, location. Does cannula site affect AID performance? | Diabettech - Diabetes and Technology
Rotate your injection or infusion sites. That's a key message that anyone living with type 1 is delivered very early in their life with the condition. And for good reason. Nobody wants to have to live with scar tissue or lipohypertrophy affecting their insulin absorption. But within the advice...
www.diabettech.com
As the article mentions, the sample size was small but it could be interesting wrt where to inject (yes, the article talks about pumps but absorption issues maybe the same with injections) and the different insulin profiles.
- Status
- This thread is now closed. Please contact Anna DUK, Ieva DUK or everydayupsanddowns if you would like it re-opened.